O ferro é um elemento importante para várias funções fundamentais do corpo, uma das quais, capacidade cognitiva, é fundamental para os geeks.
Além disso, o ferro regula vários processos, alguns dos quais são mostrados na figura.
No artigo, descobriremos quais são as causas do desequilíbrio de ferro, quais testes devem ser tomados para controle e como manter seu nível na faixa normal.

Homeostase do ferro
, [1].
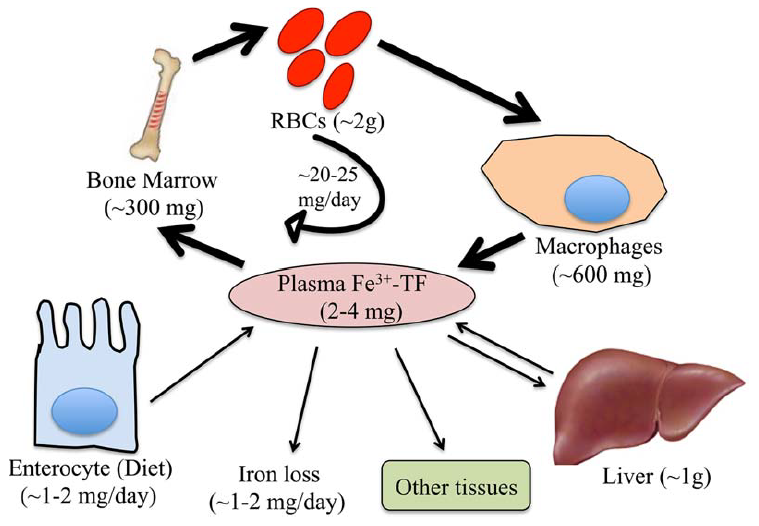
. 1. . (Fe) , (TF) ( , ).
(RBCs), , .
.
, [1].
(2 ) .
( 60% 80% ).
.
(2–4 ). , ( ) (20–25 ).
1–2 , 1–2 , , .
, -, , - .
, [1].
( ).
, , 50 % [2].
, , , .
, , ( ), , , (, ), ( , ) [1].
(, , , , – ( ) [3]) ( ) .
, , [4,5].
, , ().
, .
, . , , .
, .
- , .
, , [1].
, , ( ) .
.
( , )[6].
, , .
, ()- () . , , , [7].
, 1930- - 2-4 , 1 ( — , ).
, . -, .
.
[8].
, .
, .
(SF) (TST) (. 2):
1) , , . , - , . , .
2) β- , 1, .
1. [8].
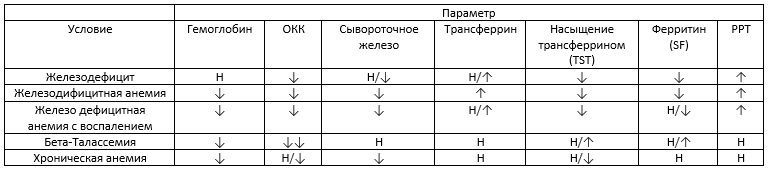
– , – , ↓ -, ↑ — , ↓↓ — , — .
3) SF TST : (1) SF > 100 / TST 20–50%; (2) SF > 100 / TST < 20%; (3) SF < 30 / TST < 20%.
4) - .
5) . ( 3), . , () . , - .
6) . . — , [9]. , . . .
(.)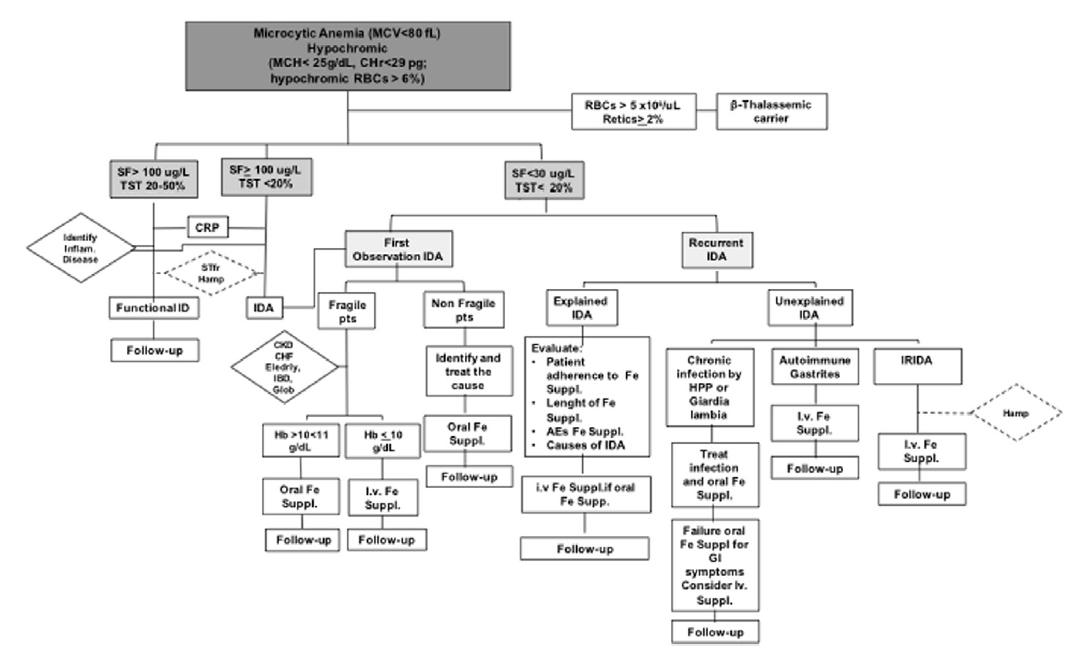
. 2. [9].
:
- , . — .
- , , , .
- (30-100 ) ( 2) .
- () .
- , ( ) . , , .
2. [8]. 1 .
/, , .
, . , , .
, , , , . .
, .
( 3).
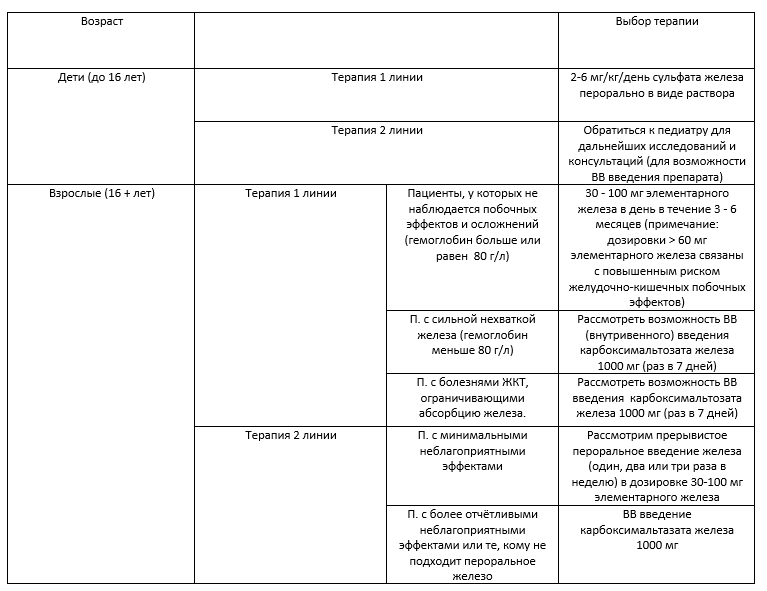
3. [8]

.
– 10 – 30 ( 4).
4. .
, , , , . .
, , .
, , , , - , .
, , , , , .
, , , . C- ( , ) , , , .
, .
, .
.
Lifext ,
, . , .
Lifext.
— + .
, Google. Lifext, . ( ) + .
— 120. ( 1,9$, ). , . - , , .
, , ;)


-
[1] S. Dev, J.L. Babitt, Overview of iron metabolism in health and disease, Hemodial. Int. 21 (2017) S6–S20. doi:10.1111/hdi.12542.
[2] E. McLean, M. Cogswell, I. Egli, D. Wojdyla, B. De Benoist, Worldwide prevalence of anaemia, WHO Vitamin and Mineral Nutrition Information System, 1993-2005, Public Health Nutr. 12 (2009) 444–454. doi:10.1017/S1368980008002401.
[3] P. Guggenbuhl, Y. Deugnier, J.F. Boisdet, Y. Rolland, A. Perdriger, Y. Pawlotsky, G. Chalès, Bone mineral density in men with genetic hemochromatosis and HFE gene mutation, Osteoporos. Int. 16 (2005) 1809–1814. doi:10.1007/s00198-005-1934-0.
[4] A.L. Fracanzani, D. Conte, M. Fraquelli, E. Taioli, M. Mattioli, A. Losco, S. Fargion, Increased cancer risk in a cohort of 230 patients with hereditary hemochromatosis in comparison to matched control patients with non-iron-related chronic liver disease, Hepatology. 33 (2001) 647–651. doi:10.1053/jhep.2001.22506.
[5] C. Borgna-Pignatti, G. Vergine, T. Lombardo, M.D. Cappellini, P. Cianciulli, A. Maggio, D. Renda, M.E. Lai, A. Mandas, G. Forni, A. Piga, M.G. Bisconte, Hepatocellular carcinoma in the thalassaemia syndromes, Br. J. Haematol. 124 (2004) 114–117. doi:10.1046/j.1365-2141.2003.04732.x.
[6] A. Poujois, J.C. Devedjian, C. Moreau, D. Devos, P. Chaine, F. Woimant, J.A. Duce, Bioavailable Trace Metals in Neurological Diseases, Curr. Treat. Options Neurol. 18 (2016). doi:10.1007/s11940-016-0426-1.
[7] M.J. Murray, A.B. Murray, M.B. Murray, C.J. Murray, The adverse effect of iron repletion on the course of certain infections, Br. Med. J. 2 (1978) 1113–1115. doi:10.1136/bmj.2.6145.1113.
[8] M.S.Y. Low, G. Grigoriadis, Iron deficiency and new insights into therapy, Med. J. Aust. 207 (2017) 81–87. doi:10.5694/mja16.01304.
[9] L. De Franceschi, A. Iolascon, A. Taher, M.D. Cappellini, Clinical management of iron deficiency anemia in adults: Systemic review on advances in diagnosis and treatment, Eur. J. Intern. Med. 42 (2017) 16–23. doi:10.1016/j.ejim.2017.04.018.