Besi adalah elemen penting untuk sejumlah fungsi tubuh mendasar, salah satunya, kemampuan kognitif, sangat penting bagi Geeks.
Selain itu, zat besi mengatur sejumlah proses, beberapa di antaranya ditunjukkan dalam gambar.
Dalam artikel ini, kami akan mencari tahu apa penyebab ketidakseimbangan besi, tes apa yang harus diambil untuk kontrol, dan bagaimana mempertahankan levelnya dalam kisaran normal.

Homeostasis besi
, [1].
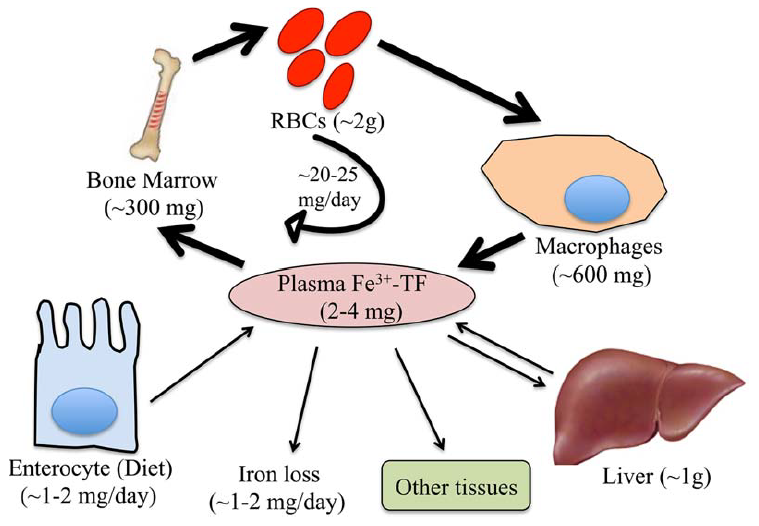
. 1. . (Fe) , (TF) ( , ).
(RBCs), , .
.
, [1].
(2 ) .
( 60% 80% ).
.
(2–4 ). , ( ) (20–25 ).
1–2 , 1–2 , , .
, -, , - .
, [1].
( ).
, , 50 % [2].
, , , .
, , ( ), , , (, ), ( , ) [1].
(, , , , – ( ) [3]) ( ) .
, , [4,5].
, , ().
, .
, . , , .
, .
- , .
, , [1].
, , ( ) .
.
( , )[6].
, , .
, ()- () . , , , [7].
, 1930- - 2-4 , 1 ( — , ).
, . -, .
.
[8].
, .
, .
(SF) (TST) (. 2):
1) , , . , - , . , .
2) β- , 1, .
1. [8].
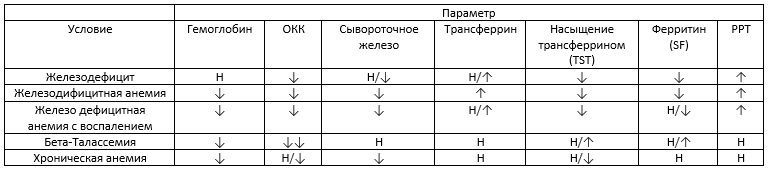
– , – , ↓ -, ↑ — , ↓↓ — , — .
3) SF TST : (1) SF > 100 / TST 20–50%; (2) SF > 100 / TST < 20%; (3) SF < 30 / TST < 20%.
4) - .
5) . ( 3), . , () . , - .
6) . . — , [9]. , . . .
(.)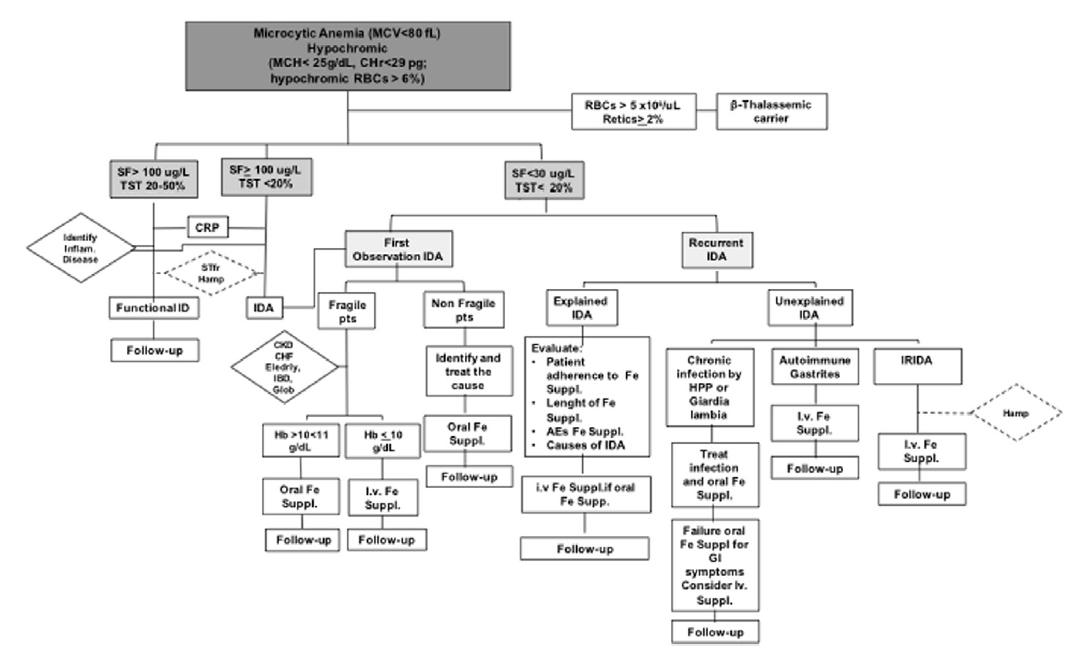
. 2. [9].
:
- , . — .
- , , , .
- (30-100 ) ( 2) .
- () .
- , ( ) . , , .
2. [8]. 1 .
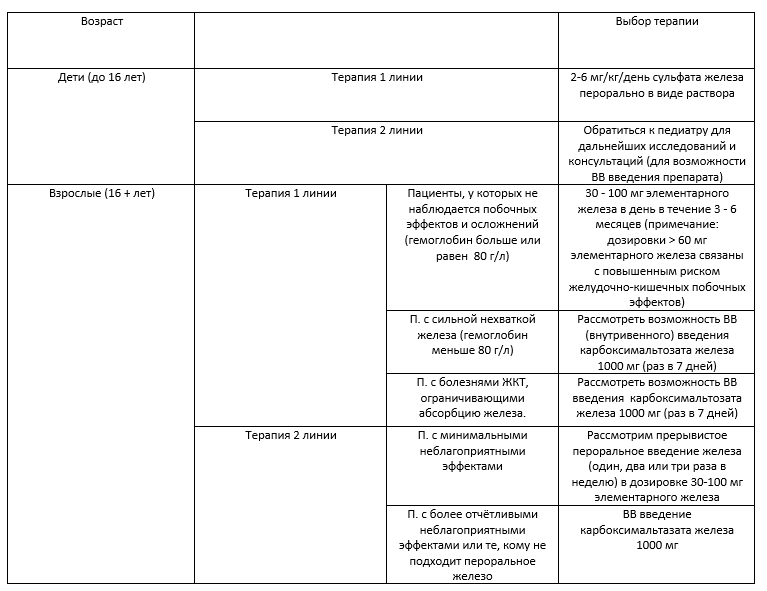
/, , .
, . , , .
, , , , . .
, .
( 3).
3. [8]

.
– 10 – 30 ( 4).
4. .
, , , , . .
, , .
, , , , - , .
, , , , , .
, , , . C- ( , ) , , , .
, .
, .
.
Lifext ,
, . , .
Lifext.
— + .
, Google. Lifext, . ( ) + .
— 120. ( 1,9$, ). , . - , , .
, , ;)


-
[1] S. Dev, J.L. Babitt, Overview of iron metabolism in health and disease, Hemodial. Int. 21 (2017) S6–S20. doi:10.1111/hdi.12542.
[2] E. McLean, M. Cogswell, I. Egli, D. Wojdyla, B. De Benoist, Worldwide prevalence of anaemia, WHO Vitamin and Mineral Nutrition Information System, 1993-2005, Public Health Nutr. 12 (2009) 444–454. doi:10.1017/S1368980008002401.
[3] P. Guggenbuhl, Y. Deugnier, J.F. Boisdet, Y. Rolland, A. Perdriger, Y. Pawlotsky, G. Chalès, Bone mineral density in men with genetic hemochromatosis and HFE gene mutation, Osteoporos. Int. 16 (2005) 1809–1814. doi:10.1007/s00198-005-1934-0.
[4] A.L. Fracanzani, D. Conte, M. Fraquelli, E. Taioli, M. Mattioli, A. Losco, S. Fargion, Increased cancer risk in a cohort of 230 patients with hereditary hemochromatosis in comparison to matched control patients with non-iron-related chronic liver disease, Hepatology. 33 (2001) 647–651. doi:10.1053/jhep.2001.22506.
[5] C. Borgna-Pignatti, G. Vergine, T. Lombardo, M.D. Cappellini, P. Cianciulli, A. Maggio, D. Renda, M.E. Lai, A. Mandas, G. Forni, A. Piga, M.G. Bisconte, Hepatocellular carcinoma in the thalassaemia syndromes, Br. J. Haematol. 124 (2004) 114–117. doi:10.1046/j.1365-2141.2003.04732.x.
[6] A. Poujois, J.C. Devedjian, C. Moreau, D. Devos, P. Chaine, F. Woimant, J.A. Duce, Bioavailable Trace Metals in Neurological Diseases, Curr. Treat. Options Neurol. 18 (2016). doi:10.1007/s11940-016-0426-1.
[7] M.J. Murray, A.B. Murray, M.B. Murray, C.J. Murray, The adverse effect of iron repletion on the course of certain infections, Br. Med. J. 2 (1978) 1113–1115. doi:10.1136/bmj.2.6145.1113.
[8] M.S.Y. Low, G. Grigoriadis, Iron deficiency and new insights into therapy, Med. J. Aust. 207 (2017) 81–87. doi:10.5694/mja16.01304.
[9] L. De Franceschi, A. Iolascon, A. Taher, M.D. Cappellini, Clinical management of iron deficiency anemia in adults: Systemic review on advances in diagnosis and treatment, Eur. J. Intern. Med. 42 (2017) 16–23. doi:10.1016/j.ejim.2017.04.018.