Le fer est un élément important pour un certain nombre de fonctions fondamentales du corps, dont l'une, la capacité cognitive, est essentielle pour les geeks.
De plus, le fer régule un certain nombre de processus, dont certains sont illustrés sur l'image.
Dans cet article, nous découvrirons quelles sont les causes du déséquilibre en fer, quels tests effectuer pour le contrôle et comment maintenir son niveau dans la plage normale.

Homéostasie du fer
, [1].
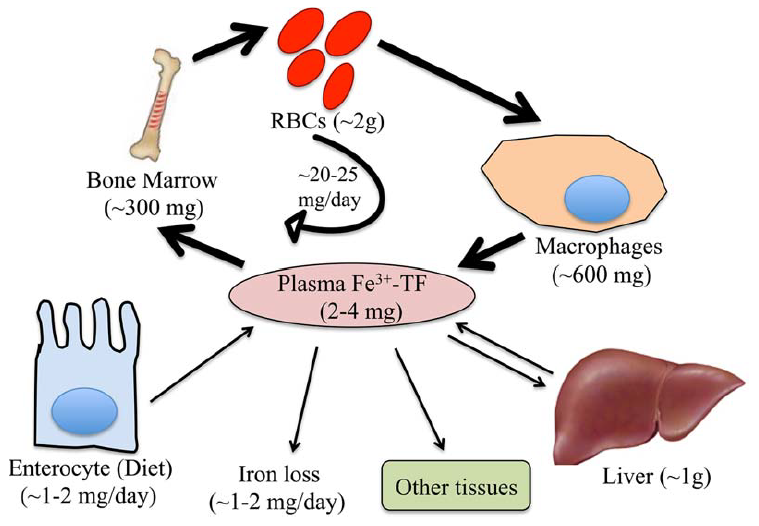
. 1. . (Fe) , (TF) ( , ).
(RBCs), , .
.
, [1].
(2 ) .
( 60% 80% ).
.
(2–4 ). , ( ) (20–25 ).
1–2 , 1–2 , , .
, -, , - .
, [1].
( ).
, , 50 % [2].
, , , .
, , ( ), , , (, ), ( , ) [1].
(, , , , – ( ) [3]) ( ) .
, , [4,5].
, , ().
, .
, . , , .
, .
- , .
, , [1].
, , ( ) .
.
( , )[6].
, , .
, ()- () . , , , [7].
, 1930- - 2-4 , 1 ( — , ).
, . -, .
.
[8].
, .
, .
(SF) (TST) (. 2):
1) , , . , - , . , .
2) β- , 1, .
1. [8].
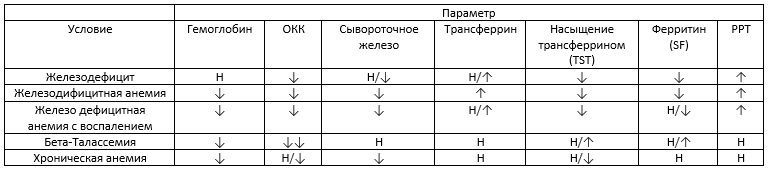
– , – , ↓ -, ↑ — , ↓↓ — , — .
3) SF TST : (1) SF > 100 / TST 20–50%; (2) SF > 100 / TST < 20%; (3) SF < 30 / TST < 20%.
4) - .
5) . ( 3), . , () . , - .
6) . . — , [9]. , . . .
(.)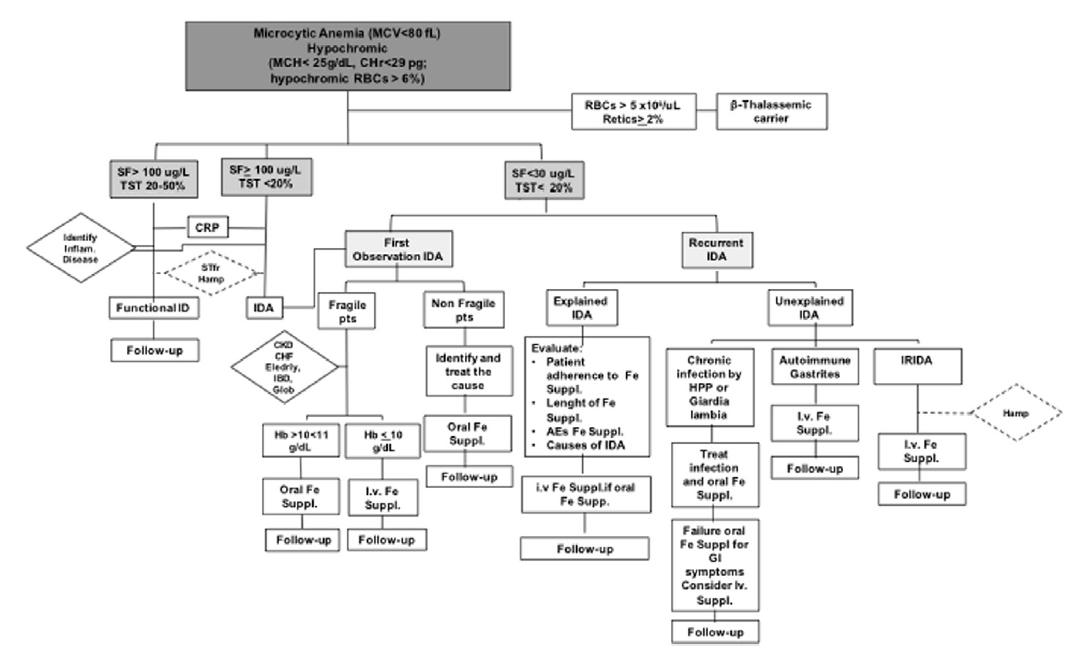
. 2. [9].
:
- , . — .
- , , , .
- (30-100 ) ( 2) .
- () .
- , ( ) . , , .
2. [8]. 1 .
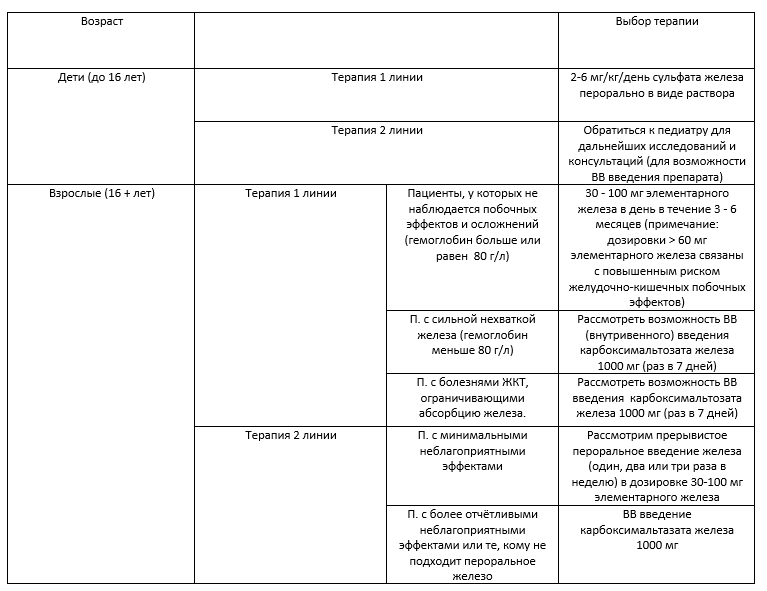
/, , .
, . , , .
, , , , . .
, .
( 3).
3. [8]

.
– 10 – 30 ( 4).
4. .
, , , , . .
, , .
, , , , - , .
, , , , , .
, , , . C- ( , ) , , , .
, .
, .
.
Lifext ,
, . , .
Lifext.
— + .
, Google. Lifext, . ( ) + .
— 120. ( 1,9$, ). , . - , , .
, , ;)


-
[1] S. Dev, J.L. Babitt, Overview of iron metabolism in health and disease, Hemodial. Int. 21 (2017) S6–S20. doi:10.1111/hdi.12542.
[2] E. McLean, M. Cogswell, I. Egli, D. Wojdyla, B. De Benoist, Worldwide prevalence of anaemia, WHO Vitamin and Mineral Nutrition Information System, 1993-2005, Public Health Nutr. 12 (2009) 444–454. doi:10.1017/S1368980008002401.
[3] P. Guggenbuhl, Y. Deugnier, J.F. Boisdet, Y. Rolland, A. Perdriger, Y. Pawlotsky, G. Chalès, Bone mineral density in men with genetic hemochromatosis and HFE gene mutation, Osteoporos. Int. 16 (2005) 1809–1814. doi:10.1007/s00198-005-1934-0.
[4] A.L. Fracanzani, D. Conte, M. Fraquelli, E. Taioli, M. Mattioli, A. Losco, S. Fargion, Increased cancer risk in a cohort of 230 patients with hereditary hemochromatosis in comparison to matched control patients with non-iron-related chronic liver disease, Hepatology. 33 (2001) 647–651. doi:10.1053/jhep.2001.22506.
[5] C. Borgna-Pignatti, G. Vergine, T. Lombardo, M.D. Cappellini, P. Cianciulli, A. Maggio, D. Renda, M.E. Lai, A. Mandas, G. Forni, A. Piga, M.G. Bisconte, Hepatocellular carcinoma in the thalassaemia syndromes, Br. J. Haematol. 124 (2004) 114–117. doi:10.1046/j.1365-2141.2003.04732.x.
[6] A. Poujois, J.C. Devedjian, C. Moreau, D. Devos, P. Chaine, F. Woimant, J.A. Duce, Bioavailable Trace Metals in Neurological Diseases, Curr. Treat. Options Neurol. 18 (2016). doi:10.1007/s11940-016-0426-1.
[7] M.J. Murray, A.B. Murray, M.B. Murray, C.J. Murray, The adverse effect of iron repletion on the course of certain infections, Br. Med. J. 2 (1978) 1113–1115. doi:10.1136/bmj.2.6145.1113.
[8] M.S.Y. Low, G. Grigoriadis, Iron deficiency and new insights into therapy, Med. J. Aust. 207 (2017) 81–87. doi:10.5694/mja16.01304.
[9] L. De Franceschi, A. Iolascon, A. Taher, M.D. Cappellini, Clinical management of iron deficiency anemia in adults: Systemic review on advances in diagnosis and treatment, Eur. J. Intern. Med. 42 (2017) 16–23. doi:10.1016/j.ejim.2017.04.018.